Spring Term Clinic
A Record!
WEEK 1 - 07/01/2013
A relatively quiet first week back in term time clinic.....they are starting us off gently!
A new patient on Tuesday was relatively straightforward, a 34 year old research nurse with upper thoracic and right shoulder discomfort. I would have liked to have been grilled more by Mr Cook on my differentials and diagnosis, which was of mid thoracic facilitation and compensatory torsion through the right shoulder giving hypertonic and ischaemic musculature. My patient had quite a stressful job which was mostly desk based and I wanted to try and get her breathing pattern corrected (she was very much an upper rib breather) and stretch out her anterior structures and hip flexors. I had a feeling that when she left clinic the patient wouldn't return.....not because she was dissatisfied but because she had been reassured that her symptoms weren't anything more sinister and she was happy to try the exercises I'd given her. Watch this space!
An interesting returning patient on Thursday prompted a discussion with Mr Michaels on how best to treat a kyphotic / lordotic patient with extension through the T/L region. Mr Michaels explained that the best way to stretch this area without extending it further would be with supine rotational stretches, using the patient's breathing to increase the stretch. Essentially he was trying to make me think more three dimensionally rather than simply through the anterior/posterior plane. This is something I know I need to work on.
A new patient on Tuesday was relatively straightforward, a 34 year old research nurse with upper thoracic and right shoulder discomfort. I would have liked to have been grilled more by Mr Cook on my differentials and diagnosis, which was of mid thoracic facilitation and compensatory torsion through the right shoulder giving hypertonic and ischaemic musculature. My patient had quite a stressful job which was mostly desk based and I wanted to try and get her breathing pattern corrected (she was very much an upper rib breather) and stretch out her anterior structures and hip flexors. I had a feeling that when she left clinic the patient wouldn't return.....not because she was dissatisfied but because she had been reassured that her symptoms weren't anything more sinister and she was happy to try the exercises I'd given her. Watch this space!
An interesting returning patient on Thursday prompted a discussion with Mr Michaels on how best to treat a kyphotic / lordotic patient with extension through the T/L region. Mr Michaels explained that the best way to stretch this area without extending it further would be with supine rotational stretches, using the patient's breathing to increase the stretch. Essentially he was trying to make me think more three dimensionally rather than simply through the anterior/posterior plane. This is something I know I need to work on.
Week 2 - 14/01/2013
3 new patients this week, very pleased!
Patient 1 - presenting with a 5 year history of intermittent left lateral knee pain which is progressing to left lateral hip, thigh and calf pain. The patient had surgery on a left hallux valgus 5 years ago and had 3 tendons severed at the same time to assist with hammer toes - the patient didn't know which muscle tendons were involved but it looks like it was probably extensor digitorum longus or brevis.
I have not had a kneee patient in a very long time and although structurally I feel confident with this area I know that functionally I could improve and I really need to revise gait mechanics. With the onset, surgery history of the patient and the progressive picture of symptoms there is surely a compensatory picture in evidence. This presentation also highlights that I need to have a stronger understanding of exercise rehabilitation. Next time the patient is in clinic I want to start assessing from the head down, rather than focusing on just the focal area.
Patient 2 - this one really threw me! A 40 year old male cafe worker presenting with low back pain, worse on the left with bilateral radiations to the buttocks and lateral thighs down to but not below the knees. History of a similar episode a year previously and with a recent history of 2 slight falls on to the buttocks. So far not too bad....I had a few differentials: ankylosing spondylitis, facet, segmental strain, sacro-iliac joint strain.
However! the clinicial testing confused me: positive straight leg raise test on the left, crossed straight leg raise test on the right, reduced L5/S1 reflex on the left, bilateral absent pin prick test over S1 dermatome. I would have thought that this would strongly indicate a discal strain or even prolapse, however active movement in to flexion was unrestricted and pain free. There were also no obvious palpatory findings in terms of tenderness but there was quite marked muscular hypertonicity through the lower lumbars and gluteii. On discussion with Fiona Walsh it was thought that the picture was still indicative of a deep structure, probably a disc being the cause of the local and radiating pain although I couldn't quite bring all my findings together and if that had been a CCA patient I think I could have dug myself a very deep hole. A good patient to have pre CCA though.
Patient 3 - another low back pain patient. This was a 28yr old lady, mother of a 7yr old daughter with left sided low back pain and radiations to left buttock, and lateral thigh and leg down to the heel. The onset was a week previously and there was a 3 year history of similar episodes. The presenting picture and clinical findings were much easier to correlate with this patient: reduced lumbar flexion which brought on the back and leg pain, positive SLRT on left, not on right, reflexes were normal bilaterally. Passively the lumbar movement was segmentally restricted at L1/2 and lower thoracic spine and the SIJ was restricted on the left but asymptomatic. I diagnosed an anular strain at L5/S1.
Possibly because I had had a similar patient earlier in the week, possibly because the clinical testing provided less 'confusing' results, I found this much easier to understand and by the end of the session I thought I had quite a good grasp of the patient and had presented it well. I had good feedback from both Mr Michaels and my 2 observers too, always a bonus!
Patient 1 - presenting with a 5 year history of intermittent left lateral knee pain which is progressing to left lateral hip, thigh and calf pain. The patient had surgery on a left hallux valgus 5 years ago and had 3 tendons severed at the same time to assist with hammer toes - the patient didn't know which muscle tendons were involved but it looks like it was probably extensor digitorum longus or brevis.
I have not had a kneee patient in a very long time and although structurally I feel confident with this area I know that functionally I could improve and I really need to revise gait mechanics. With the onset, surgery history of the patient and the progressive picture of symptoms there is surely a compensatory picture in evidence. This presentation also highlights that I need to have a stronger understanding of exercise rehabilitation. Next time the patient is in clinic I want to start assessing from the head down, rather than focusing on just the focal area.
Patient 2 - this one really threw me! A 40 year old male cafe worker presenting with low back pain, worse on the left with bilateral radiations to the buttocks and lateral thighs down to but not below the knees. History of a similar episode a year previously and with a recent history of 2 slight falls on to the buttocks. So far not too bad....I had a few differentials: ankylosing spondylitis, facet, segmental strain, sacro-iliac joint strain.
However! the clinicial testing confused me: positive straight leg raise test on the left, crossed straight leg raise test on the right, reduced L5/S1 reflex on the left, bilateral absent pin prick test over S1 dermatome. I would have thought that this would strongly indicate a discal strain or even prolapse, however active movement in to flexion was unrestricted and pain free. There were also no obvious palpatory findings in terms of tenderness but there was quite marked muscular hypertonicity through the lower lumbars and gluteii. On discussion with Fiona Walsh it was thought that the picture was still indicative of a deep structure, probably a disc being the cause of the local and radiating pain although I couldn't quite bring all my findings together and if that had been a CCA patient I think I could have dug myself a very deep hole. A good patient to have pre CCA though.
Patient 3 - another low back pain patient. This was a 28yr old lady, mother of a 7yr old daughter with left sided low back pain and radiations to left buttock, and lateral thigh and leg down to the heel. The onset was a week previously and there was a 3 year history of similar episodes. The presenting picture and clinical findings were much easier to correlate with this patient: reduced lumbar flexion which brought on the back and leg pain, positive SLRT on left, not on right, reflexes were normal bilaterally. Passively the lumbar movement was segmentally restricted at L1/2 and lower thoracic spine and the SIJ was restricted on the left but asymptomatic. I diagnosed an anular strain at L5/S1.
Possibly because I had had a similar patient earlier in the week, possibly because the clinical testing provided less 'confusing' results, I found this much easier to understand and by the end of the session I thought I had quite a good grasp of the patient and had presented it well. I had good feedback from both Mr Michaels and my 2 observers too, always a bonus!
Week 3 - 21/01/2013
A relatively quiet week in clinic this week, a few continuation patients but no new patients.
On the spur of the moment I asked Linda Goddard if she would come in to one of my continuation patients as a CCA examiner and let's just say it didn't go well! I couldn't think of answers to even the most simple questions! How do corticosteroids work? How can temporal arteritis be a clinical emergency? The list goes on.....the thing is I know this, I just panicked! Ah well, at least I know I have LOTS of revision to do.
On the spur of the moment I asked Linda Goddard if she would come in to one of my continuation patients as a CCA examiner and let's just say it didn't go well! I couldn't think of answers to even the most simple questions! How do corticosteroids work? How can temporal arteritis be a clinical emergency? The list goes on.....the thing is I know this, I just panicked! Ah well, at least I know I have LOTS of revision to do.
Week 4 - 28/01/2013
It's getting busy! I seem to have lots of continuation patients booked in with me this week, that I haven't seen before. That's fine....but there seem to be lots of people with no patients, so I'm not sure what the theory is behind this. It's all good practice though so I shouldn't complain.
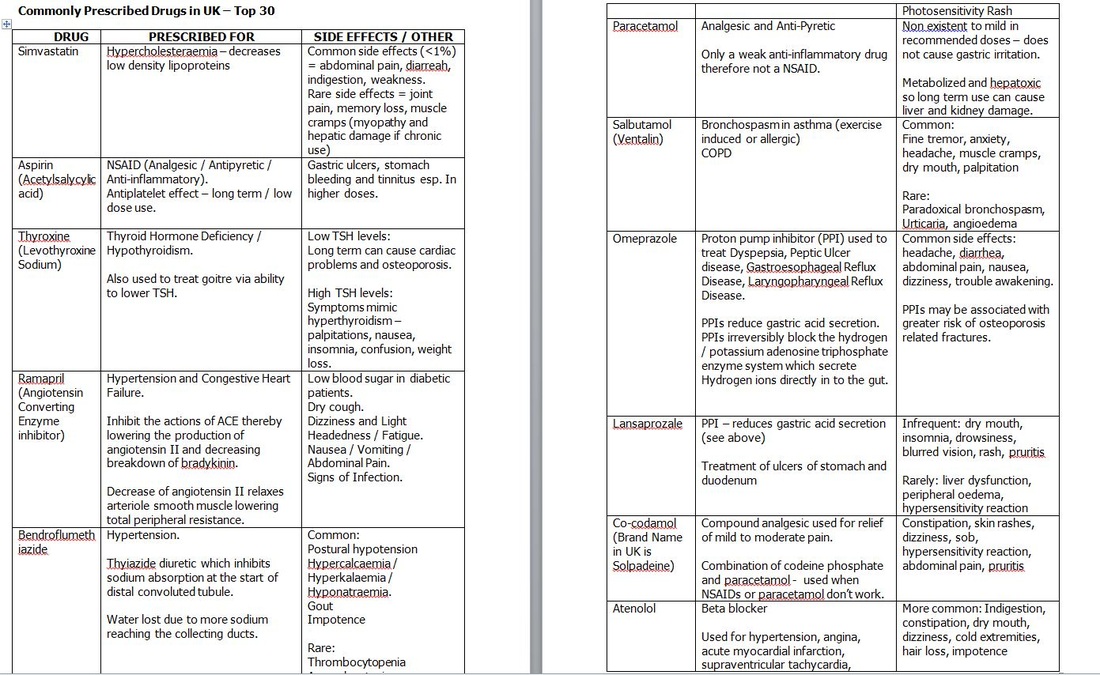
I also prepare my handout for the tutorial on pharmacology and the Top 30 drugs prescribed by GPs, based on number of prescriptions given. It's really, really useful doing this, for some reason it makes it much more manageable when you think about how commonly prescribed some drugs are and being able to recognise their names. I've always found remembering pharmacology quite a challenge - must be my dread of all things Chemistry!
Several of my team 4 colleagues have told me how useful they found the handout and they have it for easy reference in their clinic folders, which is really nice to hear.
I also prepare my handout for the tutorial on pharmacology and the Top 30 drugs prescribed by GPs, based on number of prescriptions given. It's really, really useful doing this, for some reason it makes it much more manageable when you think about how commonly prescribed some drugs are and being able to recognise their names. I've always found remembering pharmacology quite a challenge - must be my dread of all things Chemistry!
Several of my team 4 colleagues have told me how useful they found the handout and they have it for easy reference in their clinic folders, which is really nice to hear.
Week 7 - 18/02/2013
I had a very interesting new patient on Tuesday and I hope not an indicator of the imminently approaching CCA! The lady was 30 minutes late arriving and so I only had time for the case history. Even with 45 minutes I struggled to fit the case history in as my patient was very, very chatty. The patient presented with pain from cervical spine to buttock on the right with diffuse neurological symptoms in to the right upper and lower extremity and symptoms that were there "24 hours a day" although this later seemed to change. All the symptoms, together with undiagnosed depression and "many years of confusion and forgetfulness" seemed to stem from an accident on a bus several years previously. The patient also complained of shortness of breath, anxiety, urgency incontinence, nocturia and tiredness. Unfortunately we didn't have time for an examination so the patient is due to return next week.
I presented the patient at the tutorial on Thursday and in hindsight, I really should have been a lot more thorough with some of my questioning. For example, I didn't ask the patient more about the incontinence or about the tiredness etc. I think because the patient was quite eccentric and hard to control I had written her off as "eccentric" and probably an unreliable witness. Whilst I think elements of that are true I do realise that I made some mistakes. For example I didn't link the nocturia and urgency incontinence with the possibility of fibroids or a uterine mass and so I wouldn't have thought of doing an abdominal exam. I'm sure this wouldn't have been a good CCA patient. The take home message: Be More Inquisitive.....why does the patient have the symptoms!
I presented the patient at the tutorial on Thursday and in hindsight, I really should have been a lot more thorough with some of my questioning. For example, I didn't ask the patient more about the incontinence or about the tiredness etc. I think because the patient was quite eccentric and hard to control I had written her off as "eccentric" and probably an unreliable witness. Whilst I think elements of that are true I do realise that I made some mistakes. For example I didn't link the nocturia and urgency incontinence with the possibility of fibroids or a uterine mass and so I wouldn't have thought of doing an abdominal exam. I'm sure this wouldn't have been a good CCA patient. The take home message: Be More Inquisitive.....why does the patient have the symptoms!
Week 8 - 25/02/2013
Monday - a busy day, fully booked, with 3 patients I had not seen before.
First patient up is an inquisitive and intelligent man with sternal and rib pain who has also been diagnosed with toxiplasmosis. He's not really responding to the treatment he's previously received and he wants to know why......fair enough really! I don't feel I know his presentation well enough to answer that question and so end up saying that some people take longer to respond than others and we'll give it a couple more treatments before re-assessing. I feel he's not happy with that reply and I can understand, I am not sure how else I could have responded though. I'll need to re-read his notes again before next week.
The second patient was a 35yr old man with cerebral palsy. It is quite a severe cerebral palsy and at first it's difficult to understand his speech and it's certainly quite difficult to treat him due to the uncontrolled movement but it's really interesting and I do feel at the end of the session there is some tissue quality change.
Also today is the return of my new patient from last week - she seems less manic than last week, which is a relief. I perform a respiratory, CVS, abdominal and full neurological exam. Nothing untoward comes to light, although there is some sensory loss over the L2 and C2 distributions bilaterally and the abdominal exam does reveal some tenderness on Murphy's point. The patient has previously been diagnosed with fibromyalgia and many of the symptoms do fit this diagnosis. I also think that the patient's poor posture and some degenerative changes in the cervical spin are contributing to the symptoms. We write a letter to the patient's GP for them to do some further testing for possible underlying endocrinological causes for the nocturia and tiredness.
First patient up is an inquisitive and intelligent man with sternal and rib pain who has also been diagnosed with toxiplasmosis. He's not really responding to the treatment he's previously received and he wants to know why......fair enough really! I don't feel I know his presentation well enough to answer that question and so end up saying that some people take longer to respond than others and we'll give it a couple more treatments before re-assessing. I feel he's not happy with that reply and I can understand, I am not sure how else I could have responded though. I'll need to re-read his notes again before next week.
The second patient was a 35yr old man with cerebral palsy. It is quite a severe cerebral palsy and at first it's difficult to understand his speech and it's certainly quite difficult to treat him due to the uncontrolled movement but it's really interesting and I do feel at the end of the session there is some tissue quality change.
Also today is the return of my new patient from last week - she seems less manic than last week, which is a relief. I perform a respiratory, CVS, abdominal and full neurological exam. Nothing untoward comes to light, although there is some sensory loss over the L2 and C2 distributions bilaterally and the abdominal exam does reveal some tenderness on Murphy's point. The patient has previously been diagnosed with fibromyalgia and many of the symptoms do fit this diagnosis. I also think that the patient's poor posture and some degenerative changes in the cervical spin are contributing to the symptoms. We write a letter to the patient's GP for them to do some further testing for possible underlying endocrinological causes for the nocturia and tiredness.
